
Cutaneous lupus erythematosus (CLE) was first described in dogs in 1979. Isolated cases have also been reported in cats. CLE represents a group of autoimmune diseases with various clinical manifestations, in which the immune system targets the animal’s own skin cells. CLE is divided into two groups: lupus-associated dermatitis and lupus-nonspecific dermatitis. The lupus- associated dermatoses include subacute cutaneous lupus erythematosus (SCLE) and chronic cutaneous lupus erythematosus (CCLE). Acute cutaneous lupus erythematosus (ACLE) has so far only been described in humans. Diseases in the lupus-associated group typically present with skin lesions only, while laboratory findings are generally unremarkable. Lupus-nonspecific dermatitis, on the other hand, can occur as a cutaneous manifestation of systemic lupus erythematosus (SLE), a condition that affects internal organs (see Fig. 2).
Lupus-Associated Dermatitis
Vesicular Cutaneous Lupus Erythematosus (VCLE)
Vesicular cutaneous lupus erythematosus (VCLE) is classified as a subtype of subacute cutaneous lupus erythematosus (SCLE) and occurs primarily in Collies and Shelties.
Clinical Signs
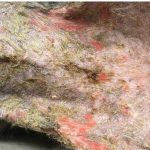
Erythematous, exudative, serpiginous or polycyclic erosions, as well as ulcerative dermatitis, may appear in the axillae, inguinal region, medial thighs, pinnae, oral cavity, and mucocutaneous junctions (see Fig. 1). The disease is not primarily associated with pruritus, although itching may develop secondary to frequent bacterial infections.
VCLE can follow a relapsing course, with clinical signs often worsening during the summer months. In some cases, spontaneous remission has been reported. The most important differential diagnosis is erythema multiforme, as the clinical presentation can be very similar. Systemic signs are typically absent in dogs with VCLE.

Diagnosis
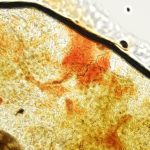
The diagnosis is based on clinical symptoms combined with histopathological examination.
Treatment
Affected patients should be protected from sunlight. Secondary infections must be excluded cytologically. Prednisolone at a dosage of 2 mg/kg/day is frequently recommended as an effective monotherapy. If lesions do not sufficiently regress, zathioprine at 2 mg/kg/day can be added.
Cyclosporine (5–10 mg/kg/day) may also be used, although its onset of action takes 2–4 weeks.
Therefore, glucocorticoids are typically combined during the initial weeks of treatment. Additionally, topical application of 0.1% tacrolimus ointment can be used.
Chronic cutaneous lupus erythematosus (CCLE)
The category of chronic cutaneous lupus erythematosus (CCLE) includes exfoliative cutaneous lupus erythematosus (ECLE), mucocutaneous lupus erythematosus (MCLE), and discoid cutaneous lupus erythematosus (DLE). DLE is further subdivided into facial discoid lupus erythematosus (FDLE) and generalized discoid lupus erythematosus (GDLE).
Exfoliative cutaneous lupus erythematosus (ECLE)
Exfoliative cutaneous lupus erythematosus was first described in German Shorthaired Pointers and later in Magyar Vizslas. Due to clinical similarities with sebadenitis, misdiagnosis can occur.
Clinical symptoms
The most common clinical signs are scaling, alopecia, and follicular casts (keratin collars around hair shafts). Ulcerations and crusts may also be present. ECLE may occur with or without pruritus. Lesions are frequently located on the muzzle, ears, back, and abdomen. Systemic signs such as joint pain, lameness, fever, and lymphadenopathy have been observed in some affected dogs. Blood chemistry and urinalysis are generally normal. In isolated cases, thrombocytopenia and mild anemia have been reported.
Diagnosis
The diagnosis is based on clinical symptoms combined with histopathological examination.
Treatment
Due to the limited efficacy of immunomodulatory drugs, ECLE represents the most challenging form of cutaneous lupus erythematosus to treat. Cyclosporine, glucocorticoids, azathioprine, and leflunomide can be administered as monotherapy or in combination but are often ineffective. Consequently, more than half of the patients in previous studies were ultimately euthanized due to lack of therapeutic response.
There are some reports of successful use of alternative medications such as mycophenolate mofetil and high-dose oclacitinib in ECLE patients. Mycophenolate mofetil was successfully used in a German Shorthaired Pointer. High-dose oclacitinib (1.8 mg/kg/day) was described as an effective monotherapy in two reports involving a total of three patients. Notably, complete remission was achieved in a Magyar Vizsla treated with high-dose oclacitinib despite prior unsuccessful treatment with cyclosporine. Therefore, oclacitinib has been suggested as a possible standard monotherapy. However, another report documented the death of a female dog after four months of therapy with oclacitinib.
Mucocutaneous Lupus Erythematosus (MCLE)
Mucocutaneous lupus erythematosus (MCLE) has been described in German and Belgian Shepherd dogs of various ages. The primary differential
diagnosis is mucocutaneous pyoderma.
Clinical symptoms
Ulcerative lesions commonly occur symmetrically in mucocutaneous areas. The perianal and perigenital regions are most frequently affected. Additionally, ulcers may appear on the lips or around the eyes (Fig. 3 and 4). Due to the ulcerative lesions in the perianal or perigenital region, these patients are often presented because of painful defecation or urination. Pruritus is generally absent or only mild in intensity.

Diagnosis
Since mucocutaneous pyoderma is the primary differential diagnosis, it should be excluded by cytological examination. Moreover, mucocutaneous pyoderma typically resolves with antibiotic therapy, which is not the case in MCLE patients. The diagnosis should be confirmed by histopathological examination.
Treatment
The prognosis for MCLE is good, and treatment with prednisolone (2 mg/kg/day) can lead to rapid healing within one month. One report described successful use of oclacitinib in two MCLE patients.
Discoid Lupus Erythematosus (DLE)
Discoid lupus erythematosus (DLE) is the most common form of lupus in this category and is divided into two groups: facial or localized discoid lupus erythematosus (FDLE), in which skin lesions are confined to the head and neck, and generalized discoid lupus erythematosus (GDLE), where lesions also occur below the neck. The disease can occur at any age. Since most cases are worsened or possibly even triggered by UV light exposure, the condition was formerly referred to as nasal solar dermatitis or photosensitive nasal lupus.
Clinical Symptoms
The clinical signs of facial discoid lupus erythematosus (FDLE) typically begin with depigmentation, erythema, and scaling on the nose. These lesions can progress to erosions, ulcerations, crusts, and loss of the normal architecture of the planum nasale; the nasal bridge may also be affected (Fig. 5 and 6). Over time, these changes can spread to other sun-exposed areas such as the lips, pinnae, and periocular region. Patients with generalized discoid lupus erythematosus (GDLE) may additionally show generalized or multifocal plaques and alopecia on the neck, back, and thorax. Both FDLE and GDLE can present with or without pruritus. Both forms of the disease are usually benign and do not exhibit systemic involvement.

Diagnosis
The diagnosis is based on the patient’s history, clinical signs, and histopathological examination.
Therapy
Patients ‒ like those with VCLE ‒ should be protected from sunlight, as UV exposure worsens symptoms. Topical tacrolimus ointment (0.1%) as monotherapy can be effective. If the response is
insufficient, glucocorticoids combined with tacrolimus ointment may be administered. Cyclosporine is also an option. Successful treatment with oclacitinib has been reported in four dogs with FDLE.
Lupus-unspecific Dermatitis
Systemic lupus erythematosus (SLE) is a multisystem disease with diverse symptoms but lacks the histopathological features typical of cutaneous lupus erythematosus (CLE). Reported signs in SLE patients include joint disease, haematologic abnormalities, glomerulonephritis, ulcerative stomatitis, and fever. Dermatologic manifestations such as scaling, mucocutaneous and oral ulcers, ulceration and/or hyperkeratosis of the paw pads, and alopecia may also occur. The prognosis is generally poor.
Dr. Amir Davoodi
Our services related to lupus diseases:
- Large screening + complete blood count
- Cytology
- Histopathology
Further literature:
Olivry T, Linder KE, Banovic F. Cutaneous lupus erythematosus in dogs: a comprehensive review. BMC Vet Res. 2018 Apr 18;14(1):132
Miller WH, Griffin CE, Campbell KL. Muller and Kirk’s small animal dermatology. Elsevier Health Sciences; 2012.
Noli C, Scarampella F, Toma S. Praktische Dermatologie bei Hund und Katze: Klinik-Diagnose-Therapie. Schlütersche; 2014.
Harvey RG, Olivrī A, Lima T, Olivry T. Effective treatment of canine chronic cutaneous lupus erythematosus variants with oclacitinib: Seven cases. Vet Dermatol. 2023 Feb;34(1):53-58.

{kind=link}