
{kind=link}
Columnaris disease in koi and aquarium fish
The causative agent of columnaris disease is Flavobacterium columnare, a bacterium that plays a particularly important role in the ornamental fish trade. Flavobacterium columnare is a Gram- negative, rod-shaped bacterium measuring 5–12 × 0.5 μm. It exhibits slow gliding motility but lacks flagella. Flavobacterium columnare has been detected in popular aquarium fish species such as neon tetra (Paracheirodon innesi), platy (Xiphophorus maculatus) and zebrafish (Danio rerio), as well as in pond fish such as koi (Cyprinus carpio). In principle, the pathogen can occur in all freshwater fish; however, outbreaks in pond fish are most common during the summer months when water temperatures are higher. Entry points for the pathogen are skin lesions. Infection is further promoted by poor water quality, high ammonia concentrations, elevated pH, and low oxygen levels. Initially, small whitish lesions develop around the mouth, fin margins, and scales, which resemble fungal growth as they enlarge. In scaleless fish such as channel catfish (Ictalurus punctatus), the infection begins as small bluish-grey necrotic lesions in the skin with a reddish inflammatory margin.
Microscopically, large numbers of F. columnare bacteria can be detected both in the centre and at the wound margins, with the edge often appearing to consist almost entirely of bacterial cells. In fish with scales, lesions may begin at the outer fin margins and spread inwards across the body, giving a saddle-like appearance. This is the origin of the term “saddleback disease”. Initially, degradation of the fin edges occurs, leaving the fin rays exposed. The gills may also be affected. In such cases, the gill lamellae disintegrate from the tips towards the gill arches. In juvenile fish, excessive swelling of the gill epithelium and increased mucus production often lead to adhesion of the gill lamellae. The consequence is reduced oxygen uptake, resulting in rapid respiratory movements.
Two clinical forms of columnaris disease can be distinguished. In the chronic form, white lesions enlarge slowly and fish die only after a prolonged course of disease. In the acute form, skin lesions spread within hours. Up to 50% of a fish population may die within 36 hours. In experimental infections in zebrafish, characteristic dorsal lesions have been observed as early as 24 hours post infection. Treatment must therefore be initiated rapidly.

Antibiotic treatment based on antibiogram results is generally possible. However, it should always be combined with optimisation of husbandry conditions. As the pathogen prefers an alkaline environment, lowering the pH to 6.8 may support treatment. For diagnosis, a swab is taken from affected body areas. This can be examined both by culture and by PCR. On Anacker–Ordal agar, F. columnare grows as pale yellow colonies at 18–30 °C (Fig. 1), with a tendency to adhere to the agar surface. At temperatures below 14 °C and above 33 °C, no growth occurs under culture conditions.
Cultural examination allows for antimicrobial susceptibility testing (antibiogram). The advantage of PCR lies in a shorter turnaround time and significantly higher sensitivity through DNA detection. In addition, a small piece of affected fin tissue can be excised and examined microscopically. This reveals that many columnaris bacteria attach at one end and exhibit oscillating movements with the free end. At the margins of inflamed tissue areas, they aggregate into column-like or cluster-like structures.
Emydomyces testavorans – a cutaneous fungus in turtles
Emydomyces testavorans is a keratinophilic fungus found in freshwater turtles. It belongs to the order Onygenales, which also includes other reptile- associated pathogens such as the genera Nannizziopsis, Ophidiomyces and Paranannizziopsis, all of which are primarily associated with dermatological diseases in various reptile species.
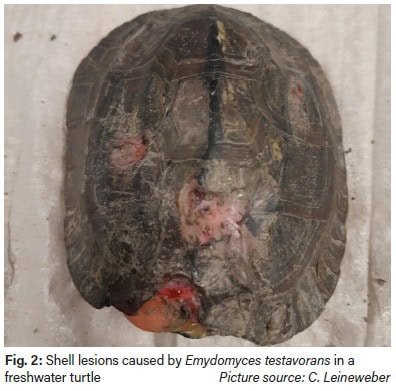
Emydomyces testavorans was first described in association with ulcerative shell lesions in freshwater turtles in the western United States (Woodburn et al. 2019). Since then, it has been detected in several species in North America (Woodburn et al. 2019; Davidson et al. 2025; Brunner et al. 2024; Fredrickson et al. 2024). To date, all research and reported detections of E. testavorans originate exclusively from North America, where the fungus has been identified in both zoological collections and wild freshwater turtle populations. Clinically and pathologically, ulcerative shell lesions are most commonly described (Fig. 2), which may also affect deeper shell structures. In severe cases, epithelial inclusion cysts may develop and extend into deeper tissues; these can be visualised using computed tomography. In milder cases, pale areas on the shell may be observed. Chronic disease courses with slowly progressive shell changes have also been reported. Histologically, affected animals may show squamous epithelial metaplasia, hyperkeratosis, inflammation, and osteonecrosis (Woodburn et al. 2021).
Treatment is challenging and prolonged, and includes antifungal therapy, particularly terbinafine, as well as regular cleaning and disinfection of the environment. Effective disinfectants appear to include chlorine bleach, chlorhexidine, and accelerated hydrogen peroxide (Liszka et al. 2025). Diagnosis of Emydomyces testavorans is often difficult. The detection of characteristic inclusion cysts in the shell using computed tomography may indicate infection in severe cases. However, the fungus is difficult to culture and is often overgrown by other environmental or shell-associated fungi in culture. Superficial lesions frequently no longer contain viable fungal elements, and sampling from deeper layers can be challenging.
The recommended sample for pathogen detection by PCR is a combined swab from the oropharynx, cloaca, and shell. A dry swab (without transport medium) should be used. Recently, Laboklin has established a PCR assay for the detection of Emydomyces testavorans, making diagnosis of this pathogen possible in Europe. In recent months, several detections have already been made in different freshwater turtles in Germany, indicating that the pathogen is present in Europe and may cause clinical disease.
Dr. Martin Felten, Dr. Christoph Leineweber, Dr. Rachel Marschang